
Compiled by Bose Ravenel MD (pediatrician retired)

https://www.theblaze.com/op-ed/horowitz-the-science-of-remdesivir-vs-ivermectin-a-tale-of-two-drugs
Horowitz: The $cience of remdesivir vs. ivermectin: A tale of two drugs
OP-ED DANIEL HOROWITZ October 18, 2021

A tale of two drugs. One has become the standard of care at an astronomical cost despite studies showing negative efficacy, despite causing severe renal failure and liver damage, and despite zero use outpatient.
| Original Investigation Infectious Diseases July 15, 2021 Association of Remdesivir Treatment With Survival and Length of Hospital Stay Among US Veterans Hospitalized With COVID-19 Michael E. Ohl, MD, MSPH1,2; Donald R. Miller, ScD3,4; Brian C. Lund, PharmD1; et alTakaaki Kobayashi, MD1,2; Kelly Richardson Miell, PhD1; Brice F. Beck, MA1; Bruce Alexander, PharmD1; Kristina Crothers, MD5,6; Mary S. Vaughan Sarrazin, PhD1,2 Author Affiliations Article Information JAMA Netw Open. 2021;4(7):e2114741. doi:10.1001/jamanetworkopen.2021.14741 Conclusions and Relevance In this cohort study of US veterans hospitalized with COVID-19, remdesivir treatment was not associated with improved survival but was associated with longer hospital stays. Routine use of remdesivir may be associated with increased use of hospital beds while not being associated with improvements in survival. |
The other has been safely administered to billions for river blindness and now hundreds of millions for COVID throughout the world and has turned around people at death’s doorstep for pennies on the dollar. Yet the former – remdesivir – is the standard of care forced upon every patient, while the latter – ivermectin – is scorned and banned in the hospitals and de facto banned in most outpatient settings. But according to the NIH, a doctor has the same right to use ivermectin as to use remdesivir. And it’s time people know the truth.
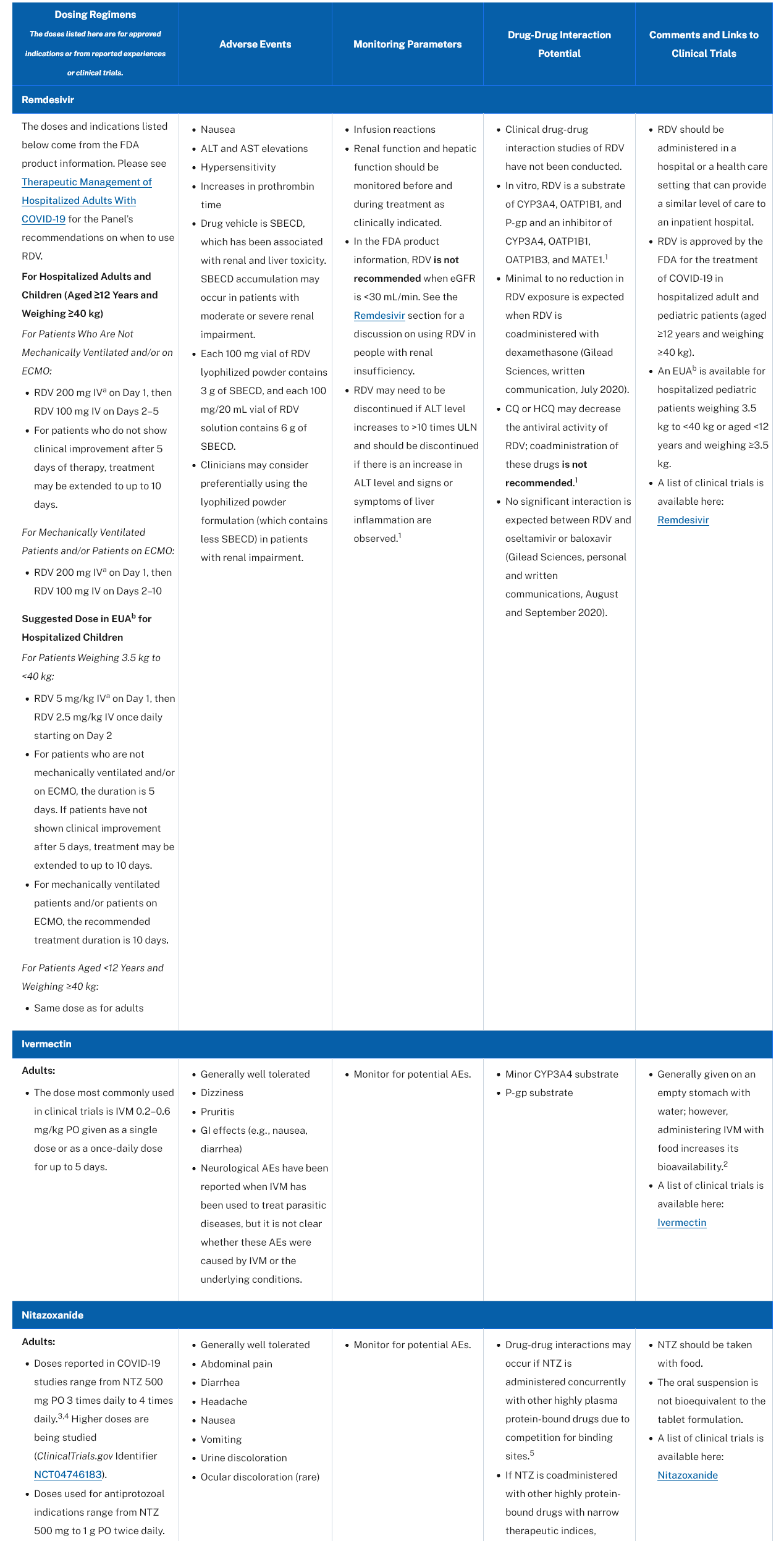
Although the NIH and the FDA didn’t officially approve ivermectin as standard of care for COVID, it is listed on NIH’s website right under remdesivir as “Antiviral Agents That Are Approved or Under Evaluation for the Treatment of COVID-19.” It is accorded the same status, the same sourcing for dosage recommendations, and the same monitoring advice as remdesivir … except according to NIH’s own guidance, remdesivir has a much greater potential for severe reactions in the very organs at stake in a bout with acute COVID.
| https://www.covid19treatmentguidelines.nih.gov/tables/table-2e Table 2e. Characteristics of Antiviral Agents That Are Approved or Under Evaluation for the Treatment of COVID-19 Last Updated: July 8, 2021 |
Now, let’s take a closer look at the details.
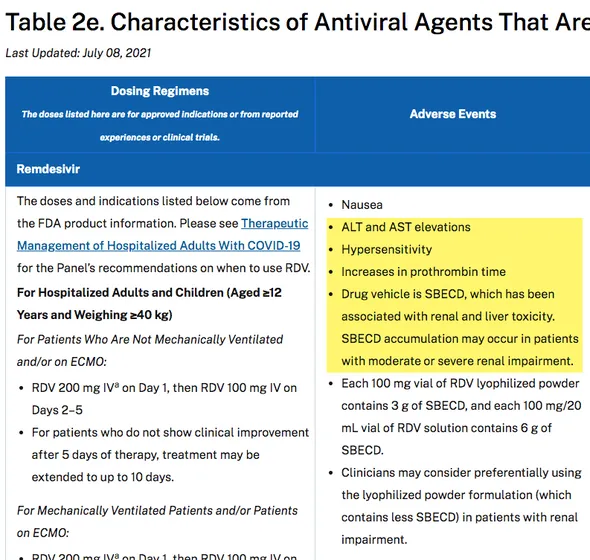
As you can see, they admit that remdesivir causes renal and liver failure! One of the symptoms is “ALT and AST elevations,” which are indications of liver damage. Is that really the drug you want when someone is at risk for a cytokine storm and thrombosis? They even have a monitoring requirement for these side effects. Also, it does have some drug interactions as well.
Now, let’s move on to the ivermectin side effects.
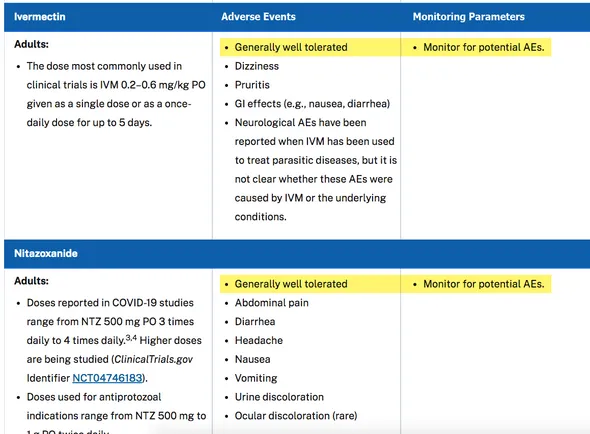
Notice how the NIH is essentially saying it has no side effects by the fact that it prefaces the section by noting the drug is “generally well tolerated,” a distinction not accorded to remdesivir. Then it proceeds to list the same boilerplate GI and nausea warnings on every drug under the sun. There are almost no drug interactions and ZERO specific guidance for monitoring!
Just looking at the NIH’s own table, why in the world would remdesivir be the expensive mandatory standard of care and ivermectin, buttressed by 64 studies, be relegated to hemlock status even for patients about to die and with no other options?
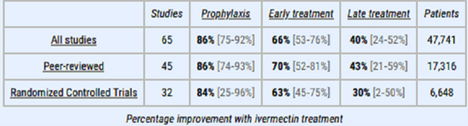
| https://www.theblaze.com/op-ed/horowitz-new-study-shows-denial-of-ivermectin-is-a-crime-against-humanity Until now, despite dozens of studies and doctors all around the world with no financial gain at stake vouching for its efficacy, our government has balked at ivermectin because, it claims, the studies are too small. Well, the Argentinian Provincial Ministry of Health just published the results of a retrospective study of a trial of over 21,000 participants. The results were unmistakable among those participants above age 40, all non-vaccinated. Overall, when adjusting for confounding factors like less healthy people joining the ivermectin group, those in the ivermectin group had a 66% lower ICU admission rate and a 55% lower mortality rate than those in the control group. Anyone in the ivermectin group was treated with a dose of 0.6mg per kg of weight one time a day for five days. This is just the latest study, but the key is to look at the preponderance of the evidence. A meta-analysis posted earlier this week of 65 total studies netted the following pooled results. |
Yes, we get the message – every one of those studies is supposedly low-powered, a fraud, and all the thousands of doctors turning people around on ivermectin are somehow frauds even though they have nothing to gain and everything to lose from pushing it. But if that is our standard for ivermectin, it raises the obvious question about remdesivir. How could remdesivir not only be approved but made the standard of care when it has negative efficacy in trials, has a negative recommendation from the WHO, and, by the NIH’s own admission, causes liver and kidney failure?
| https://www.who.int/news-room/feature-stories/detail/who-recommends-against-the-use-of-remdesivir-in-covid-19-patients WHO recommends against the use of remdesivir in COVID-19 patients 20 November 2020 |
Even if the medical establishment dismisses the preponderance of evidence and reality of the past 18 months, with ivermectin saving so many people, just from a safety standpoint, why would they not allow people to at least try something this safe while forcing on them a dangerous drug like remdesivir? In addition, these are the same hospitals that administer Olumiant, which has a rare FDA black box warning for blood clots, even though these very patients are at high risk for a pulmonary embolism and other clotting disorders?
In other words, there is no way anyone can justify the war on ivermectin (and every other cheap treatment that has been and will be proposed) as being rooted in anything related to medicine and science. If that were the case, the medical establishment would be dead set against remdesivir and Olumiant. Moreover, to the extent remdesivir has any efficacy that is worth its risk, it would be outpatient during the viral stage. There is quite literally no scientific way remdesivir can work in the pulmonary inflammation stage. Unlike ivermectin, which tones down inflammatory cytokines such as IL-1beta and IL-10 as well as tumor necrosis factor alpha, remdesivir has no anti-inflammatory qualities.
However, remdesivir does have a lot of political science behind it. Aside from having the weight of Big Pharma pushing it (and it was concocted by UNC-Chapel Hill, curiously the same institution at the center of the coronavirus gain-of-function research), hospitals get a 20% bonus for using it!
Gee, is there any wonder hospitals will fight patients in court – including those whom they already recommend to remove from life support – to not even try ivermectin as a last resort?! So much for the desire to flatten the curve of hospitalizations. They want people in the hospital! If they really cared about the run on hospitals, they’d promote treatments that work early and outpatient so that nobody would need to come to the hospital.
For more information, watch this devastating contrast of ivermectin vs. remdesivir.
Here’s one other strong piece of evidence that this is not about any shortcoming of ivermectin, but stems from unrelenting war on anything off patent that might work, in order to run interference for expensive, dangerous, and ineffective tools of big pharma. Let’s go back to that NIH chart of potential antiviral drugs for COVID. There is actually a third one on that list aside from remdesivir and ivermectin.
Here’s one other strong piece of evidence that this is not about any shortcoming of ivermectin, but stems from unrelenting war on anything off patent that might work, in order to run interference for expensive, dangerous, and ineffective tools of big pharma. Let’s go back to that NIH chart of potential antiviral drugs for COVID. There is actually a third one on that list aside from remdesivir and ivermectin.
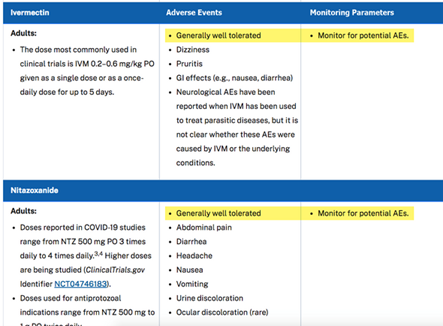
Nitazoxanide, much like ivermectin, is a (potentially) cheap off-patent anti-parasitic that has been praised for years as a very safe, broad-spectrum anti-parasitic mechanism and is written about glowingly in studies. And it actually has an even longer and more direct precedent of research and clinical use against viruses than even ivermectin. It is the standard of care for norovirus and rotavirus in Brazil and has shown promise against not just flus and hepatitis, but coronavirus colds, SARS, and MERS. This research has been known even in the media for well over a year! Gee, we have an antiviral that is so safe it’s given to young kids for viral diarrhea and has been known to work against coronaviruses. Yet our government has refused to pursue any meaningful research for 18 months!
Originally, it was as cheap as ivermectin, but one company seems to have bought it up, and now it is prohibitively expensive in the U.S. However, were the government to promote it, this off-patent drug could easily be mass-produced for pennies on the dollar and costs just a few dollars for a full regimen in Mexico and Brazil.
Notice that, just like with ivermectin, the NIH prefaces the side effects section on nitazoxanide by saying it is “generally well tolerated” and then proceeds to list the boilerplate of typical minor side effects that are disclosed for every drug under the sun. Anyone merely looking at this NIH page alone can see how the government and medical establishment’s treatment of remdesivir vs. every other therapeutic that has been tried is built upon control, greed, and something much darker than that. Now, just remember, these are the same people who will look you in the eye and say the shots are 100% effective and carry zero risk. It’s all in the $cience.
What is self-evident from the NIH’s disclosure, which was updated as late as July 2021, is that ivermectin and nitazoxanide work for a lot more than just parasites. It’s primarily the political parasites that fear those drugs.

