
North Carolina Commission for Public Health November 2, 2022
1931 Mail Service Center
Raleigh, NC 27699
Dear Commission Member:
We are writing regarding the recent decision by the CDC’S Advisory Committee on Immunization Practices (ACIP) to include approved or authorized Covid-19 vaccines in the Recommended Childhood Vaccine schedule beginning Jan 1, 2023. We are concerned that the Commission for Public Health might consider requiring this vaccine for school attendance in the state of North Carolina.
Please be advised that North Carolina Physicians for Freedom (NCPFF) is a network comprised of several hundred physicians and other types of health care practitioners within our state. We strongly oppose requiring that this vaccine be imposed upon North Carolina children and adolescents for school attendance.
NCPFF bases this recommendation upon the following considerations:
- Public health requires that a rigorous, scientifically defensible risk-benefit analysis be applied. This would reveal that the risk of harm due to these vaccines for children and adolescents far outweighs any theoretical, potential benefit they might experience. The scientific record demonstrates that in less than two years, the Covid-19 vaccines have caused more severe vaccine reactions and deaths than all the other widely available vaccines combined in 30 years pre-pandemic. In addition, the risk of minors experiencing severe complications or death due to becoming infected with the SARS CoV-2 virusis minimal – less than that for seasonal influenza for current variant strains. Moreover, it is widely known that these vaccines do not reliably prevent infection or transmission. Finally, current variants are much less pathogenic than alpha and other earlier variants1-2 years ago. All these factors combined militate overwhelmingly against any public health imperative to require the vaccine. (Please refer to our attached Position Paper on this topic that contains additional technical information including data and literature references).
- Any action to require that minors in the state of North Carolina take a Covid-19 vaccine would be unconstitutional based on at least several constitutional provisions.
- Any action to require that minors in the state of North Carolina take the Covid-19 vaccine would be illegal, in part because it would be arbitrary and capricious, and lack any rational basis; and
- Any action to require this of minors in the state of North Carolina would be an actionable tort when vaccine injuries causing impairment and fatalities occur.
NCPFF requests that an exhaustive, rigorous, unbiased scientific investigation be undertaken on this issue before you consider requiring that minors receive this vaccine for school attendance.
We stand ready to assist the Commission and offer a wide range of expertise on these matters. Please feel free to contact us at dlightfoot@ncphysiciansforfreedom.com if we can be of service; we would appreciate a response as soon as possible.
Respectfully,
*The original letter was signed by 13 members of the board of directors and advisory board.
Please find attached a summary of the evidence upon which I encourage the Committee to reject any attempt to add any CoVID vaccine to the childhood recommended schedule.
I am a Medical Advisor for North Carolina Physicians for Freedom (NCPFF), a growing statewide organization of over 300 medical professionals including physicians, nurse practitioners, and others advocating for medical freedom for both medical professionals and their patients. Many of them have treated numerous patients, including many in very high-risk categories with CoVID-19 illness successfully with an emphasis upon early ambulatory treatment in the manner described in my attached summary.
The information and sources in this document were the basis for a formal Report to a domestic court in Pennsylvania just a few weeks ago during the process of my serving as an expert witness for the mother of two teenage sons seeking to allow the two young men not to take a CoVID vaccine being pushed by their father. Opposing counsel and expert witness for the father agreed to allow the boys to stand by their preference not to be vaccinated after a review of my pending testimony and this Report with embedded source references.
The information compiled in this Report is a product of my intensive study of the issues involved for an estimated 3,900 hours over the past 2 1/2 years following my retirement. I would point out that virtually every major point made is referenced, and the citations in support are from credible sources including leading medical experts, government organizations, scientists, and public health authorities,
I submit that children and adolescents are at minimal risk of serious complications of current and likely further SARS CoV-2 variants, while signals for serious adverse events of historic proportions are rapidly mounting, even in the face of the fact that the unprecedented global application of novel vaccines have not allowed sufficient time to determine long-term adverse events. All this within the context of there being available effective preventive and therapeutic measures in the event of the rare serious manifestations of CoVID-19 in this demographic group.
Thank you for your consideration.
Bose Ravenel, MD, FAAP, Retired
Colfax, North Carolina
A Critical Analysis of CoVID Vaccines for Children and Adolescents
Bose Ravenel, MD, FAAP, Retired
Biographical Note:
I am a retired pediatrician after 31 years in private practice, 11 years in academic pediatric medicine, and 6 ½ years practicing Integrative pediatric medicine. My Integrative Medicine experience involved searching for root causes for complex, chronic health problems which had been intractable to conventional medical approaches and finding safe and effective innovative treatment approaches. During my career I had a special interest in Vaccine Informed Consent and developed a 24-page referenced Vaccine Informed Consent summary for many parents of my patients who sought such information. Following retirement on March 16, 2020, I sensed some unusual aspects of the CoVID pandemic and plunged into researching this topic – having devoted an estimated 3,900 hours to the subject to date.
| Executive Summary · Children and adolescents are at negligible risk of serious illness or death from current CoVID strains. A CDC pediatrician recently (June 2022) claimed otherwise, but based the recommendation on flawed data. · CoVID-19 vaccines are unnecessary, and effective, safe, inexpensive early treatments are available. · Immunity from prior CoVID-19 in children and adolescents is more robust and longer-lasting than that from vaccines. · Adverse effects upon the immune system and tissue damage from CoVID-19 vaccines are disproportionately higher than benefits and should not be administered to healthy children and adolescents. · Current CoVID-19 vaccines do not prevent infection or transmission. · Absolute risk reduction from the vaccines is very low as opposed to relative risk reduction, which appears dramatic but is highly misleading and did not follow FDA published guidelines for communicating risks and benefits to the public. · Long-term risks for children and adolescents from these vaccines are unknown. Emergency authorization was granted by the FDA that only included studies with data accumulated over a few months. According to the Johns Hopkins University & Medicine Coronavirus Resource Center, typical vaccine development takes 5 to 10 years, although an “Accelerated Timeline” is 1-2 years in total. · Even in the face of the above limitations in safety surveillance for these vaccines, the available evidence of adverse events is historically high. The number of deaths following CoVID vaccines reported in the VAERS system in about 18 months exceeds the total number of deaths reported in the same system for all vaccines combined over the 32 years prior to the pandemic. Marked clustering of deaths closer to date of vaccination furthermore supports causality. · Vaccination increases myopericarditis risk 83-fold compared to the background rate in adolescent males, and MRI findings indicate substantial cardiac damage. · Vaccination following natural infection increases the risk of cardiac damage. · Sudden deaths among athletes have risen exponentially during the period of widespread CoVID-19 vaccine administration Jan 2021 to April 2022 compared to data from a scientific study covering 1966 to 2004. Data from cardiac surgeon Steven Gundry’s preventive cardiology practice showed an increase in 5-year heart attack risk from pre—pandemic 11% to 25% during the CoVID-19 vaccine program. CDC VAERS data showed a dramatic increase in reports of myocarditis from fewer than 162 yearly from 2010 to 2020, to 29,432 in 2021 alone and 21,563 already in the first half of 2022. · The mRNA and viral vector DNA vaccines may encode changes into the DNA of the vaccinated individual. · FERTILITY CONSIDERATIONS FROM mRNA VACCINES * Primary Covid-19 BNT162b mRNA (Pfizer) vaccination impairs semen concentration and total motile count among semen donors – according to Israeli researchers reported in the 17 June, 2022 issue of Andrology, their findings from a study of 37 semen donors (SD) on sequential measurements of sperm and semen function from pre-vaccination to T3 at 5 to 6 months following the 2nd dose of the Pfizer two-dose primary series. * Women’s reproductive function is affected in a number of ways. CoVID-19 infection and mRNA vaccines may both cause an immune response to the spike protein in both scenarios. Miscarriages, fetal deaths, and stillbirths have skyrocketed. Fertility and birth rates have dropped dramatically and correlate with CoVID jab uptake in multiple countries · Conflicting narratives about CoVID-19 vaccines between government agencies and public health authorities vs medical professionals providing early ambulatory treatment may relate to respective vested interests on the one hand and adverse consequences for questioning a vaccine-only pathway out of the pandemic on the other. · Informed consent usual practices with current Emergency Use Authorized CoVID vaccines fail to fulfill General requirements for informed consent according to Federal Regulation 45 CFR 46.116. These include disclosure of any alternative treatment that might be advantageous to the patient, a description of any reasonably foreseeable risks, and a statement that participation is voluntary with no penalty or loss of privileges consequent to declining the vaccination. Mandates with penalties or restriction of privileges clearly violate this regulation. · Conclusions Because of the above, my personal opinion is that neither rational plausibility nor empirical data support giving any child or adolescent one of the current CoVID-19 vaccines. Risks far exceed limited benefits. The CoVID vaccine program for children and teens should be suspended immediately. Until adequate studies support a vaccine or vaccines for coronaviruses, safe, effective, multi-drug and nutraceutical treatment should be widely implemented and supported rather than being suppressed. |
Negligible risk of serious illness or death
- With no early treatment, a child’s probability of surviving an infection with CoVID-19 is at least 99.998 percent[i] according to CDC data prior to March, 2021 during predominance of the alpha strain of SARS-CoV-2 when pathogenicity was higher than with current variants.
- The current prevailing strains of CoVID are less pathogenic, while more contagious, than seasonal influenza.[ii]
- A flawed May 25, 2022 preprint study was used by an official with the CDC that exaggerated the risk of death for children from COVID-19 in her presentations to CDC and U.S. FDA advisors responsible for recommending the Pfizer and Moderna vaccines for infants and young children. This flawed study was used despite the fact that on June 28, 2022 the authors published a revised version of the study after critics had questioned some of their original findings. This revised version reduced significantly the alleged number of deaths from CoVID-19 – yet still included several tactics that exaggerate CoVID deaths in children. A number of misleading interpretations of data and manipulation are discussed in a July 27, 2022 article published by the Children’s Health Defense in the Defender.[iii] It is clear that CoVID-19 is not a leading cause of death for children and adolescents.
| Summary of flawed study data exaggerating the risk of death for children from COVID-19 · During a June 17 meeting of its Advisory Committee on Immunization Practices to discuss pediatric COVID-19 vaccines in children under 5, Dr. Katherine Fleming-Dutra, a pediatrician and pediatric emergency medicine physician with the CDC, presented a table that falsely claimed COVID-19 was a leading cause of death in U.S. children. Fleming-Dutra earlier that week presented the same table during the FDA’s vaccine advisory committee meeting, along with other slides from the original U.K. study that also falsely claimed COVID-19 as a “top 5 cause of death” in children. The table illustrated the study’s claim that COVID-19 caused more than 1 million deaths in the U.S, including at least 1,433 deaths among children and young people ages 0 to 19 years old from March 1, 2020, to April 30, 2022. · The authors falsely claimed that they only counted cases where CoVID-19 was an underlying and not just contributing cause of death – but the CDC’s mortality statistics at the time, which counted only deaths where the virus was the underlying cause of death, equated to 1,088 pediatric deaths. This correction alone dropped CoVID-19 deaths down to the eighth leading cause of death, as indicated in a revised study. Additional distortions include the following: · Cumulative deaths from CoVID-19 in the UK data were compared with annualized death numbers for other causes of death. For each age group, the cumulative CoVID death rate was more than double the annualized death rate. · Kelly recreated the results of the preprint study using CDC WONDER, where COVID-19 is listed as the underlying cause of death during the time period of the original study. She then annualized the results and counted only deaths where CoVID-19 was listed as the underlying cause. This more accurate accounting showed that COVID-19 does not rank as a “leading cause of death” for young children. Among children age 1 to 4 and 5 to 9 COVID-19 ranked in a four-way tie for the 8th leading cause of death and for teenagers age 15 to 19, the 6th. · The top few causes of death far outweigh the causes further down the list, as for example among ages 1 to 4, accidents account for almost 25 times as many deaths as COVID-19 on an annualized basis. · Pre-pandemic data from 2019 instead of 2020 or 2021 were used for other causes of death to compare to those from COVID-19 in 2020 to 2022. The CDC has acknowledged that estimates of excess deaths reported during the pandemic may not be due to COVID, but rather to other effects of the pandemic – thus other cause mortality may be under-estimated. · In the revised June 28 preprint, the authors acknowledged improper calculations for COVID-19 deaths and adjusted the rankings for each age group using CDC WONDER data – and yet several tactics were still used to exaggerate COVID deaths in children. These are discussed in the Defender article. |
Vaccines are unnecessary, and effective, safe, inexpensive early treatments are available
- The CoVID vaccines are unnecessary for children and adolescents. In the case of a child with underlying pre-existing medical conditions, early, effective, safe, inexpensive treatment is available from a number of sources that can reduce the risk of hospitalization or death by 60 to 99 percent. This consists of combination therapy with either hydroxychloroquine or ivermectin combined with zinc, vitamins C and D, and one or more of several additional nutraceutical or repurposed FDA-approved drugs such as nebulized budesonide in the event of respiratory compromise. This multiple-component, sequenced, early therapy approach has been published in two leading medical journals by Dr. Peter McCullough with co-authors – the most credentialed cardiologist in the world and author of over 40 medical journal papers on CoVID-19.[iv],[v]
- Since March of 2020, Brian Tyson and George Fareed, two physicians with impeccable credentials, have been treating COVID patients of all ages in a “hot zone” area of Imperial Valley, CA using early treatment protocols. If treatment was started within 7 days of first symptoms, among over 7,000 patients treated, only 2 people were briefly hospitalized and there were no deaths.[vi] These results largely reflect treatment during the earlier CoVID variants which were more pathogenic than the most recent one.
Immunity from prior CoVID-19 in children and adolescents is more robust and longer-lasting than that from vaccines.
- A prospective cohort study of 252 family clusters of Italian children and adults following SARS-CoV-2 infection found sustained immune response in children up to 1 year after natural infection.[vii] Among all infected subjects, 96.7% were asymptomatic or mild – and yet spike receptor-binding domain (RBD) IgG antibodies persisted in all age groups for at least 12 months following infection, with higher levels among younger subjects. From 139 individuals who were tested in parallel with both anti-SARS-CoV-2-RBD IgG and Neutralizing antibodies (Nabs), the two measures had a high correlation level. Neutralizing antibodies are derived from bone marrow B cells and prevent infection of cells,
- Another study in Nature Immunology looked at the immune response to SARS-CoV-2 mild or asymptomatic infections in 91 children and 154 adults. Both antibody and cellular immunity (T cell) were compared. Spike-specific T cell responses were more than twice as high in children and were detected in many seronegative children, indicating pre-existing cross-reactive responses six months after infection, whereas relative waning occurred among the adults. The spike-specific responses were stable beyond 12 months. The authors concluded that “children generate robust, cross-reactive and sustained responses to SARS-CoV-2 with focused specificity for the spike protein.” Importantly, they noted substantial cross-reactivity against other CoV strains.[viii]
Adverse effects upon the immune system and tissue damage from CoVID-19 vaccines
Yamamoto in a Virology Journal Letter summarizes mechanisms by which immune function can be impaired from CoVID-19 vaccines and may contribute to exacerbation of CoVID-19. References to each are cited.[ix]
- N1-methylpseudouridine is used as a substitute for uracil in the genetic code. The resulting modified protein can activate regulatory T cells, resulting in decreased cellular immunity.
- The spike proteins produced in the vaccine recipient circulate throughout the body on exosomes for more than four months.
- Lipid nanoparticles (LNPs) accumulate in the liver, spleen, adrenal glands, and ovaries.
- LNP-encapsulated mRNA is highly inflammatory.
- Antibodies to the spike protein in the vaccine damage cells and tissues that are primed to produce spike proteins, and vascular endothelial cells are damaged by spike proteins in the bloodstream.
- Antibody-dependent enhancement may occur where the effect of neutralizing antibodies is reduced in preventing infection.
- The “original antigenic sin” residual immune memory of the Wuhan-type vaccine may impair the effectiveness of the vaccine against variant CoVID strains.
Current CoVID vaccines do not prevent infection or transmission
- The current CoVID vaccines do not prevent either infection of, or transmission from, vaccinated individuals.[x],[xi] A recent analysis of government data from Canada shows that the percentage of cases, hospitalizations, and deaths from CoVID-19 for the ten-day period 6/6/22 to 6/19/22 was 93, 85, and 92 percent fully vaccinated respectively.[xii]
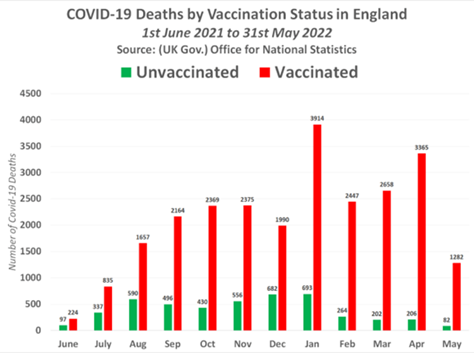
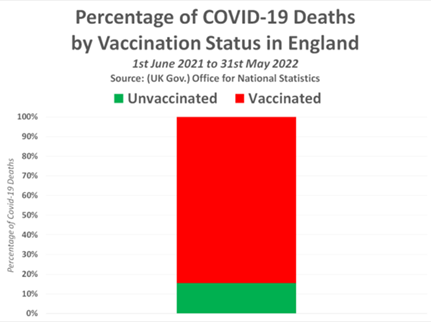
- Another study presenting CoVID-19 deaths by vaccination status from the UK Government Office for National Statistics (ONS), found dramatically higher percentages among the vaccinated than the unvaccinated for each month from 1 June 2021 to 31 May 2022. The sum total numbers for the entire period showed 84.5 percent were among the vaccinated compared with 15.5 percent unvaccinated.
- U.S. data regarding the relative proportion of CoVID cases, deaths, and hospitalizations among vaccinated vs unvaccinated individuals is compromised by differential testing and whistle-blower testimony that in some hospitals medical personnel are directed not to report deaths among vaccinated patients. At the end of May, 2021, the CDC announced the following changes in data management for CoVID-19 Case tracking:
- Routine tracking of “cases” of infection among unvaccinated only to be discontinued other than in cases of hospitalization or death.
- Routing testing for CoVID-19 with PCR based technology to be done with cycle threshold (CT) set at 28 or lower for only the vaccinated, while it would remain 37 to 40 for the unvaccinated.
| Lower CT numbers result in lower positive results. Higher CT leads to higher rates of positive. In the case of testing asymptomatic individuals, such as screening athletes or school populations, 97 to 100 percent of positives are FALSE POSITIVE. Dr. Anthony Fauci in this November 2020 interview attested to this fact. https://m.facebook.com/story.php?story_fbid=729953551198506&id=1492673654369368&refid=52&__tn__=R At 3:58 to 4:50 of a 9:06 minute video Fauci states: “If you get a cycle threshold of 35 or more that the chances of it being replication competent are miniscule . . . and . . . . you can almost never culture virus from 37 threshold cycle.” |
- Individuals who are vaccinated with one of the mRNA vaccines or the viral vector DNA vaccine (J and J) are counted as “unvaccinated” until 14 days after the final dose of the then-recommended number of doses.
Absolute risk reduction from the vaccines is very low as opposed to relative risk reduction, which appears dramatic but is highly misleading and did not follow FDA published guidelines for communicating risks and benefits to the public.
- Vaccine proponents and media almost exclusively point to the well-known claims for the Moderna Vaccine being “94.5% effective”. This figure relates to relative risk reduction.
- A simple illustration will show why Absolute risk reduction is key to understanding the practical reality of how risks of the outcome measure apply to the individual.
Assume you have a study group with 1,000 subjects who receive treatment and a control group of 1,000 who receive a placebo sham “treatment.” Assume further that 3 outcome events (i.e., CoVID cases) occur in the placebo group but only 2 in the treatment group. In this case, the relative risk reduction for the treatment group would be 2/1,000 vs 3/1,000 in the control group, or a relative risk reduction of 33.3 percent. In the case of the absolute risk reduction, 2 cases occur in the treatment group compared with 3 in the placebo group, leaving 1 case per thousand as the reduction. In other words, of the 1,000 subjects in the treatment arm, 999 derive no benefit, but all 1,000 incur whatever risks are posed from the treatment.
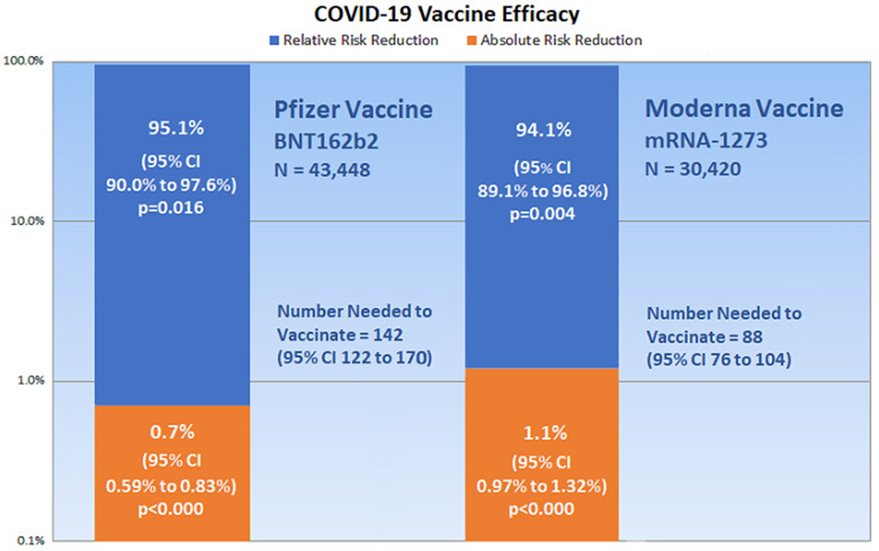
- An analysis based on data reported by the manufacturer for Pfizer/BioNTech vaccine BNT162b2, shows: relative risk reduction, 95.1%; absolute risk reduction, 0.7%. For the Moderna vaccine mRNA-1273, the appraisal shows: relative risk reduction, 94.1%; absolute risk reduction, 1.1%.[xiii] The author goes on to say:
Absolute risk reduction measures are very much lower than the reported relative risk reduction measures. Yet, the manufacturers failed to report absolute risk reduction measures in publicly released documents. As well, the U.S FDA Advisory Committee (VRBPAC) did not follow FDA published guidelines for communicating risks and benefits to the public, and the committee failed to report absolute risk reduction measures in authorizing the BNT162b2 and mRNA-1273 vaccines for emergency use. Such examples of outcome reporting bias mislead and distort the public’s interpretation of COVID-19 mRNA vaccine efficacy and violate the ethical and legal obligations of informed consent.
A graphical display of the difference between Relative Risk Reduction (RRR) and Absolute Risk Reduction (ARR) provides a powerful illustration of this vital principle:
Long-term risks for children from these vaccines are unknown.
Emergency Authorization for them was granted by the FDA following submission of data from the vaccine manufacturers that only included studies with data accumulated over a few months. According to the Johns Hopkins University & Medicine Coronavirus Resource Center, typical vaccine development takes 5 to 10 years, although an “Accelerated Timeline” is 1-2 years in total.[xiv]
Even in the face of the above limitations in safety surveillance for these vaccines, the available evidence of adverse events is historically high.
- The VAERS system is a passive reporting post-marketing safety monitoring system established in 1990. According to the Harvard Pilgrim study, fewer than 1% of vaccine adverse events are reported, 1-13% of serious events are reported for drugs and vaccines combined.[xv] Nevertheless, the number of deaths following CoVID vaccines reported in the VAERS system in about 18 months exceeds the total number of deaths reported in the same system over the 32 years prior to the pandemic. VAERS data through July 15, 2022 show 30,490 deaths following CoVID vaccines compared with 874 following all other vaccines together.[xvi] VAERS deaths following COVID-19 vaccines in the United States alone were 14,613 as of April 22, 2022.[xvii]
- The CDC and other CoVID vaccine proponents have pointed out that deaths following vaccination do not establish causality alone, but in the case of CoVID vaccines, marked clustering of the deaths closer to the day of vaccine administration strongly suggests it. VAERS data from the 4/15/2022 release of data found that 20.5% of deaths occurred within 48 hours, 30.62% within 7 days, and 53.95% within 60 days[xviii] Coincidental events would be expected to occur in a random distribution pattern from time of vaccination.
- Among serious adverse events reported following CoVID vaccines are myocarditis and pericarditis, especially among male adolescents. Although some have suggested that most of these cases of myocarditis are “mild”, Krug, Stevenson, and Hoeg reported in the European Journal of Clinical Investigation that from VAERS data, 86.9% of cases of myocarditis in adolescents were hospitalized.[xix] A Kaiser study reported the vaccine-associated rate of myo/pericarditis after the 2nd dose of vaccine at 195.4 cases/million age 12-39 years.[xx] This contrasts with a background rate of for males of 0.12-2.36 per million, age-related, lower with older age.[xxi] This equates to an 82.79-fold higher rate following the vaccines than the background rate.
- A preprint study from researchers in Thailand reported that among 301 adolescents (age 13-18,) in a prospective, cohort study following BNT162b2 (Pfizer) mRNA CoVID-19 vaccination, one developed confirmed myo/pericarditis and six more suspected myo/pericarditis during of follow-up period of just 14 days following their 2nd dose of vaccine.[xxii] This compared to a background rate from a cited study of 10 to 20 per 100,000 per year, or 0.01 to 0.02 percent per year. The authors cite another previous study that found 4.6% of subjects developed myo/pericarditis following a CoVID-19 vaccine. Overall, these researchers found evidence of cardiovascular effects in 29.24% of patients. All subjects were evaluated at days 3, 7, and 14 after their 2nd dose of vaccine with laboratory biomarkers, ECG, echocardiography, and some with cardiac MRI.
- Thirteen patients, all with severe chest pain, were described with myopericarditis, elevated troponin levels and MRI abnormalities – all within a less than a 3-month period and symptom onset less than one week following vaccination. The authors state that ”although the symptoms resolved rapidly in all patients, their CMR findings indicate the potential for myocardial fibrosis and unknown long-term impact.” [xxiii]
Vaccination following natural infection increases the risk of cardiac damage
Dr. Hooman Noorchashm, a surgeon, immunologist, and patient safety advocate, has written letters to the FDA warning that any individual who has had an infection with COVID is at higher risk of cardiac damage from the immune stimulation of a COVID vaccine and should not be vaccinated. He explains it this way:
“In the case of SARS-CoV-2, we know the virus naturally infects the heart, the inner lining of blood vessels, the lungs, and the brain, so these are likely to be some of the critical organs that will contain persistent viral antigens in the recently infected. Following reactivation of the immune system by a vaccine, these tissues can be expected to be targeted and damaged.”[xxiv]
- A scientific study published in 2006, conducted by the Division of Pediatric Cardiology, University Hospital of Lausanne, Lausanne, Switzerland, showed that there were 1,001 sudden deaths among athletes under age 35 years. This amounted to an average of 2.35 deaths per month. This compares with data from GoodSciencing.com that shows 673 deaths from Jan 2021 to April 2022 during the vaccine campaign. The monthly average is 42. Thus, we can see that 1,101 deaths occurred over 39 years, while 673 deaths occurred over 16 months during the CoVID-19 vaccine campaign.[xxv]
- Retired cardiac surgeon Dr. Steven Gundry, presented findings at the Scientific Sessions of the American Heart Association’s annual conference in Boston on November 12-14, 2021. An abstract published in Circulation, the AHA’s journal, on November 8, 2021 showed that patients in Dr. Gundry’s preventive cardiology practice had an increase in 5-year heart attack risk from 11% before the pandemic to 25%, a 227% increase, during the period of CoViD-19 vaccine uptake.[xxvi]
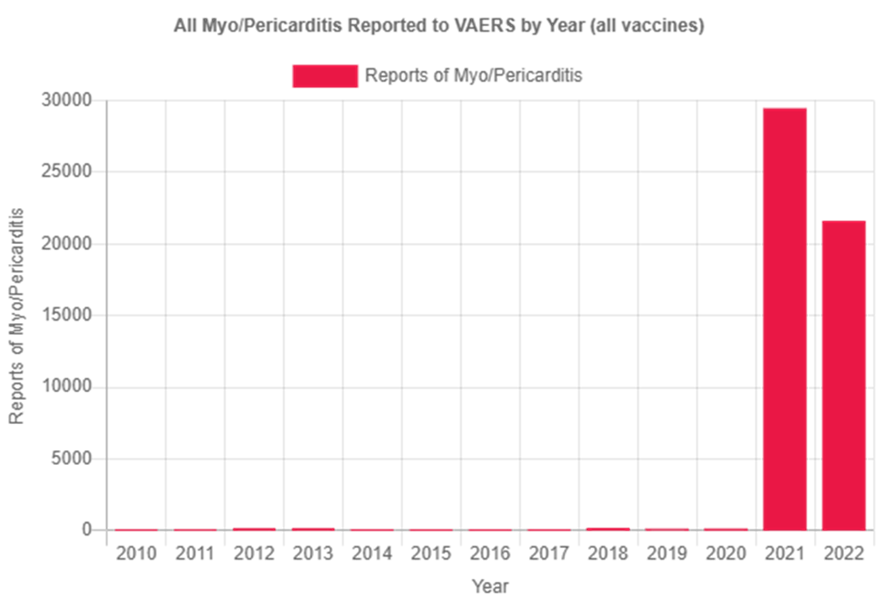
- CDC VAERS reports of myocarditis for all vaccines annually were less than 162 for each of the years from 2010 to 2020 before skyrocketing to 29,432 in 2021 and 21,563 in 2022 only up to July 22.[xxvii]
One would have to suspend rationality not to interpret the above findings as strongly suggesting a prominent role of the CoVID-19 vaccines in causing the dramatic increase in sudden deaths among athletes.
The mRNA and viral vector DNA vaccines may encode changes into the DNA of the vaccinated individual.
- A study showed that the messenger ribonucleic acid (mRNA) from the vaccine stays in the body much longer than expected. It had been expected, and depended upon, that it would not linger. It was found in lymph nodes 60 days after injection.[xxviii]
- Another study in Feb, 2022 from researchers at Lund University in Sweden found that “reverse transcription” is occurring – meaning that an enzyme makes a copy of DNA from the RNA and then integrated into the gnome of human liver cells in vitro (in a test tube). This process was found to occur within six hours of vaccine exposure.[xxix] This strongly suggests a CDC website statement that these vaccines don’t change the human genome is probably incorrect. Additional research will have to resolve this critically important question.
FERTILITY CONSIDERATIONS FROM mRNA VACCINES
Primary Covid-19 BNT162b mRNA (Pfizer) vaccination impairs semen concentration and total motile count among semen donors
- Israeli researchers reported in the 17 June, 2022 issue of Andrology, their findings from a study of 37 semen donors (SD) on sequential measurements of sperm and semen function from pre-vaccination to T3 at 5 to 6 months following the 2nd dose of the Pfizer two-dose primary series. They interpret their findings as showing significant decrease in sperm concentration in semen, sperm motility, and total motile sperm count at T2 with recovery in large measure of those decreases at T3.[xxx]
- The RAW DATA showed the following:
*Note: both median and average change in measurements are included. T3 = 5 to 6 months.
Semen Concentration: Average change from T0→T2: -15.4% Median change from T0→T2: -9,500,000 sperm per ml Average change from T0→T3: -15.9% Median change from T0→T3: -2,500,000 sperm per ml
Sperm Motility: Average change from T0→T2: -1.9%Median change from T0→T2: -5%
Average change from T0→T3: -4.1% Median change from T0→T3: +2.5%
Total Motile Count: Average change from T0→T2: -22.1% Median change from T0→T2: -27,300,000 sperm Average change from T0→T3: -19.4% Median change from T0→T3: +6,000,000 sperm
*Note: Presenting the data as median, as opposed to average, change skews the data from persisting lower numbers at T3 to a recovery from most of the loss of measures of sperm and semen function observed at T2.
- The data were obtained following only two doses of the vaccine and no boosters. It has become widely known that vaccine efficacy wanes rapidly, and boosters have been recommended, and at progressively decreasing lengths of time from completion of primary vaccination. Boosters have also been reported to be followed by more significant short-term side effects that the primary series.
- All things (above) considered, this study suggests that a reduction in male fertility from mRNA vaccines is a reasonable possibility.
Women’s reproductive function is affected in a number of ways. CoVID-19 infection and mRNA vaccines may both cause an immune response to the spike protein in both scenarios. Miscarriages, fetal deaths, and stillbirths have skyrocketed. Fertility and birth rates have dropped dramatically and correlate with CoVID jab uptake in multiple countries[xxxi]
- Four in 10 COVID-Jabbed Women Report Menstrual Irregularities
According to one recent investigation, 42% of women with regular menstrual cycles said they bled more heavily than usual after vaccination; 39% of those on gender-affirming hormone treatments reported breakthrough bleeding, as did 71% of women on long-acting contraceptives and 66% of postmenopausal women
- Menstrual Cycle Length Is Also Affected
Research published April 1, 2022, in the journal Obstetrics and Gynecology, also found an association between the COVID jab and changes in menstrual cycle length. The change was small — about one day shorter than pre-injection after the second dose
- Infection Can Suppress Ovarian Function
Some investigators have suggested the menstrual irregularities seen in female COVID patients and the COVID-jabbed alike may be attributed to an immune response to the spike protein.
- Miscarriages, Fetal Deaths, and Stillbirths Have Skyrocketed
Miscarriages, fetal deaths and stillbirths have also risen after the rollout of the COVID shots. In November 2021, Lions Gate Hospital in North Vancouver, British Columbia (BC), delivered 13 stillborn babies in a 24-hour period, and all of the mothers had received the COVID jab
- There Are No Data to Support COVID Jab for Pregnant Women
Health officials are adamant that pregnant women get a COVID-19 injection, but the data don’t support its safety. The CDC-sponsored study published in The New England Journal of Medicine (NEJM) that was widely used to support the U.S. recommendation for pregnant women to get injected was corrected in October 2021, with the correction stating:
“In the table footnotes, the following content should have been appended to the double dagger footnote:
‘No denominator was available to calculate a risk estimate for spontaneous abortions, because at the time of this report, follow-up through 20 weeks was not yet available for 905 of the 1224 participants vaccinated within 30 days before the first day of the last menstrual period or in the first trimester. Furthermore, any risk estimate would need to account for gestational week-specific risk of spontaneous abortion.’
- Massive Depopulation Underway
- Many countries are now reporting sudden declines in live birth rates, including Germany, the U.K., Taiwan, Hungary and Sweden. In the five countries with the highest COVID jab uptake, fertility has dropped by an average of 15.2%, whereas the five countries with the lowest COVID jab uptake have seen an average decline of just 4.66%
- Germany recently released data showing a 10% decline in birth rate during the first quarter of 2022.
- Other countries are also seeing unexpected birth rate reductions, nine months after the start of the mass vaccination campaign against COVID. Between January and April 2022, Switzerland’s birth rate was 15% lower than expected, the U.K.’s was down by 10% and Taiwan’s was down 23%.
- In the five countries with the highest COVID jab uptake, fertility has dropped by an average of 15.2%, whereas the five countries with the lowest COVID jab uptake have seen an average reduction of just 4.66%.
Conflicting narratives about vaccines between government agencies and public health authorities vs medical professionals providing early ambulatory treatment.
- It has become obvious even to the casual observer, that narratives about various aspects of the CoVID-19 pandemic have been sharply divergent between two groups. These are public health agencies, medical organizations, and many medical professionals on the one hand – and medical professionals who provide early ambulatory treatment for their patients who seek early treatment rather than following the advice of the CDC to avoid going to the hospital or the doctor unless and until you become sicker, on the other.
- It is prudent to consider potential vested interests on the one hand, or adverse consequences on the other – from those taking the respective sides in these conflicting narratives. In this case of CoVID vaccines, those promoting them have potential financial and/or job/career interests in recommending them. Medical and hospital system organizations often provide financial incentives for achieving certain vaccine uptake benchmarks. These are investigational medical treatments for which they have no liability in the event of adverse consequences. On the other hand, medical professionals who prefer early treatment and other measures over the vaccines as the best way to navigate through the pandemic have nothing to gain, but unprecedented adverse consequences for recommending this approach. These include possible loss of jobs or positions, and even threats of medical license suspension.
- The idea that the CDC and the FDA are not necessarily forthcoming and may not be a dependable source of information for determining which among competing narratives is true is untenable for many. As disconcerting as it is, physicians and scientists at the top levels of the NIH, FDA, and CDC have recently spoken out, expressing their frustration and alarm at the direction they see their agencies going. Some of them have spoken publicly, others have remained undisclosed due to fear of losing their job. Their concerns relate to heads of their agencies using weak or flawed data to formulate public health decisions and succumbing to political pressure emanating from the presidential administration in Washington, DC.[xxxii]
- An FDA physician expressed dissatisfaction with two developments within his agency. The first was the agency decision to authorize CoVID vaccines for infants and toddlers, even including those who had been infected with CoVID. The second was that a few months before this, the FDA bypassed their external experts to authorize booster shots for young children.[xxxiii]
- Another issue about which they were disturbed was the recommendations and even mandates, for children to wear masks in school. Studies have found that the rate of CoVID transmission was unaffected by mask wearing, and the evidence of harm has proliferated at the same time. [xxxiv] Two adjacent K-12 school districts in Fargo, North Dakota, one which had a mask mandate and one which did not in the fall of the 2021-2022 academic year were studied and no difference between masked and unmasked students could be detected.
Usual Informed Consent as related to CoVID vaccines fails to fulfill requirements of Federal Regulation. Implicit to the right to informed consent is the right to refuse a medical treatment. Many U.S. court cases have upheld the right to bodily autonomy.
- In the United States no currently available CoVID-19 vaccine is FDA approved – only Emergency Use Authorized (EUA). Therefore, they fall into the category of investigational treatments. Thus, those participating in being vaccinated are, in effect, participating in a phase 3 trial.
- Title 45 CFR 46.116 – General requirements for informed consent includes the following provisions:[xxxv]
- Disclosure of any alternative procedures or courses of treatment that might be advantageous to the subject.
- A description of any reasonably foreseeable risksor discomforts to the subject
- A statement that participation is voluntary, refusal to participate will involve no penalty or loss of benefits to which the subject is otherwise entitled.
Thus, any mandate for CoVID-19 investigational vaccines that includes any penalty or loss of privileges consequent to declining to be vaccinated violates this provision of Federal Code.
- A number of court cases settled in the United States have upheld the right to bodily autonomy and to refuse medical treatment. Several of these decisions are described in Naturopathic physician Dr. Colleen Huber’s book Neither Safe Nor Effective. The Evidence Against the CoVID Vaccines. A handful of these court decisions and opinions of judges from an essay by Ronald B. Standler covering 80 of these cases is presented with hyperlinks for easy reference for details. [xxxvi]
Dr. Robert Malone, career vaccine developer and primary creator of the platform upon which the mRNA and viral vector DNA CoVID-19 vaccines are based, warns why these vaccines should not be administered to children and adolescents.[xxxvii]
Dr. Malone:
“My name is Robert Malone, and I am speaking to you as a parent, grandparent, physician, and scientist. I don’t usually read from a prepared speech, but this is so important that I wanted to make sure that I get every single word and scientific fact correct.
I stand by this statement with a career dedicated to vaccine research and development. I’m vaccinated for COVID and I’m generally pro-vaccination. I have devoted my entire career to developing safe and effective ways to prevent and treat infectious diseases.
After this, I will be posting the text of this statement so you can share it with your friends and family.
Before you inject your child – a decision that is irreversible – I wanted to let you know the scientific facts about this genetic vaccine, which is based on the mRNA vaccine technology I created:
There are three issues parents need to understand:
The first is that a viral gene will be injected into your children’s cells. This gene forces your child’s body to make toxic spike proteins. These proteins often cause permanent damage in children’s critical organs, including
- Their brain and nervous system
- Their heart and blood vessels, including blood clots
- Their reproductive system, and
- This vaccine can trigger fundamental changes to their immune system
The most alarming point about this is that once these damages have occurred, they are irreparable
- You can’t fix the lesions within their brain
- You can’t repair heart tissue scarring
- You can’t repair a genetically reset immune system, and
- This vaccine can cause reproductive damage that could affect future generations of your family
The second thing you need to know about is the fact that this novel technology has not been adequately tested.
- We need at least 5 years of testing/research before we can really understand the risks
- Harms and risks from new medicines often become revealed many years later
Ask yourself if you want your own child to be part of the most radical medical experiment in human history
One final point: the reason they’re giving you to vaccinate your child is a lie.
- Your children represent no danger to their parents or grandparents
- It’s actually the opposite. Their immunity, after getting COVID, is critical to save your
family if not the world from this disease
In summary: there is no benefit for your children or your family to be vaccinating your children against the small risks of the virus, given the known health risks of the vaccine that as a parent, you and your children may have to live with for the rest of their lives.
The risk/benefit analysis isn’t even close.
As a parent and grandparent, my recommendation to you is to resist and fight to protect your children.”
Because of the above, my personal opinion is that neither rational plausibility nor empirical data support giving any child or adolescent one of the current CoVID-19 vaccines. Risks far exceed limited benefits. There have been more deaths (30,490 global as of July 15, 2022, with 14,613 in the U.S as of April 22, 2022) following CoVID-19 vaccines in 18 months than the total number of deaths for all vaccines reported in the same VAERS system for 32 years before the pandemic. The swine flu vaccine was pulled off the U.S. market after only 25 deaths. A study from Thailand of 301 adolescents all of whom had cardiac evaluation during 3 follow-up visits over 14 days following their 2nd dose of Pfizer mRNA vaccine found that 29% had evidence of some kind of cardiovascular effects including once case of confirmed and six more of suspected myo/pericarditis.
Vaccine mandates with any form of penalty or loss of privileges for declining to take these EUA vaccines violate Federal Code. The vaccine program applied to children and adolescents should be suspended immediately. Until adequate studies support a vaccine or vaccines for coronaviruses, safe, effective, multi-drug and nutraceutical treatment should be widely implemented and supported rather than being suppressed.
[i] https://www.cdc.gov/coronavirus/2019-ncov/hcp/planning-scenarios.html CDC COVID-19 Pandemic Planning Scenarios. Updated March 19, 2021.
[ii] https://pubmed.ncbi.nlm.nih.gov/34107134 Does Covid-19 in children have a milder course than Influenza? Kamil Yılmaz et al.Int J Clin Pract 2021 Sept;75(9):e14466.
[iii] https://childrenshealthdefense.org/defender/cdc-flawed-data-covid-shots-infants-children/?utm_source=salsa&eType=EmailBlastContent&eId=a2d4ef24-7d8f-40e0-87aa-10ac62a79d07
CDC Official Used Flawed Data to Justify COVID Shots for Infants and Children, Analysis Shows. Vegan Redshaw. The Defender July 27, 2022.
[iv] https://pubmed.ncbi.nlm.nih.gov/33387997
Multifaceted highly targeted sequential multidrug treatment of early ambulatory high-risk SARS-CoV-2 infection (COVID-19). Peter A. McCullough et. Al. Rev Cardiovasc Med. 2020 Dec 30;21(4):517-530
[v] https://www.amjmed.com/article/S0002-9343(20)30673-2/fulltext
Pathophysiological Basis and Rationale for Early Outpatient Treatment of SARS-CoV-2 Infection.
Peter A. McCullough, et al. The American Journal of Medicine, Vol 134, No 1, Jan, 2021.
[vi] Overcoming the COVID Darkness: How Two Doctors Successfully Treated 7000 Patients
by Brian Tyson, George Fareed. Feb 1, 2022.
[vii] https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2794167
Long-term Immune Response to SARS-CoV-2 Infection Among Children and Adults After Mild Infection. JAMA Netw Open. 2022;5(7):e2221616
Costanza Di Chiara, MD1 et al. July 13, 2022.
[viii]https://www.nature.com/articles/s41590-021-01089-8
Children develop robust and sustained cross-reactive spike-specific immune responses to SARS-CoV-2 infection. Alexander C. Dowell, Megan S. Butler, Shamez Ladhani. Nature Immunology 23, pages 40–49 2022.
[ix]https://virologyj.biomedcentral.com/articles/10.1186/s12985-022-01831-0#change-history
Adverse effects of COVID-19 vaccines and measures to prevent them. Kenji Yamamoto. Virology Journal, 19; June 5, 2022.
[x] https://www.cdc.gov/media/releases/2021/s0730-mmwr-covid-19.html Statement from CDC Director Rochelle P. Walensky, MD, MPH on Today’s MMWR. CDC Newsroom Media Statement. July 30, 2021.
[xi] https://www.theepochtimes.com/cdc-director-says-shes-really-struggling-with-how-to-communicate-about-covid-19_3945630.html. CDC Director Says She’s ‘Really Struggling With How to Communicate’ About COVID-19. Jack Phillips. The Epoch Times. August 12, 2021
[xii] https://expose-news.com/2022/07/20/communist-trudeau-vaccinated-92percent-covid-deaths/?cmid=c635486b-64d3-4970-a586-f798bf53617f Communist Trudeau panics after his Government reveals the Quadruple/Triple Vaccinated now account for 92% of COVID Deaths across Canada. The Expose. July 20, 2022.
[xiii] https://www.mdpi.com/1648-9144/57/3/199/htm?s=03 Outcome Reporting Bias in COVID-19 mRNA Vaccine Clinical Trials. Ronald B. Brown. Academic Editor: Edgaras Stankevičius. Medicina 2021, 57(3), 199; Published: 26 February 2021.
[xiv] https://coronavirus.jhu.edu/vaccines/timeline Typical Timeline. Johns Hopkins University & Medicine Coronavirus Resource Center. Undated.
[xv] https://digital.ahrq.gov/sites/default/files/docs/publication/r18hs017045-lazarus-final-report-2011.pdf Grant Final Report Electronic Support for Public Health–Vaccine Adverse Event Reporting System (ESP:VAERS). Submitted to: The Agency for Healthcare Research and Quality (AHRQ) Inclusive dates: 12/01/07 – 09/30/10.
[xvi] https://openvaers.com/covid-data/mortality
Oper VAERS. Vaers COVID Vaccine Mortality Reports.
[xvii] https://pierrekory.substack.com/p/vaccine-exemption-letter-for-a-16-c85?s=r
Vaccine exemption letter for a 16-year-old camp counselor. Open Letter. Pierre Kory, MD., MPA. June 6, 2022.
[xviii]https://www.medalerts.org/vaersdb/findfield.php?TABLE=ON&GROUP1=ONS&EVENTS=ON&VAX=COVID19&DIED=Yes&STATE=NOTFR
National Vaccine Information Center. 4/15/22.
[xix] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9111575
BNT162b2 Vaccine-Associated Myo/Pericarditis in Adolescents: A Stratified Risk-Benefit Analysis. Allison Krug, Josh Stevenson, Tracy Beth Hoeg. European Journal of Clinical Investigation. 2022 May; 52(5): e13759.
[xx] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9088632
Risk of myopericarditis following COVID‐19 mRNA vaccination in a large integrated health system: A comparison of completeness and timeliness of two methods
Katie A. Sharff,et al. Pharmacoepidemiol Drug Saf. 2022 Apr 16 : 10
[xxi] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9147275
Risk of Myocarditis and Pericarditis among Young Adults following mRNA COVID-19 Vaccinations. Abdallah Alami et al. Vaccines. 5 May, 2022, 10, 722.
[xxii] https://www.preprints.org/manuscript/202208.0151/v1
Pre print. Cardiovascular Effects of the BNT162b2 mRNA COVID-19 Vaccine in Adolescents.
Suyanee Mansanguan, et al. Version 1 : Received: 7 August 2022 / Approved: 8 August 2022 / Online: 8 August 2022
[xxiii] https://www.jpeds.com/article/S0022-3476(21)00665-X/pdf
Myopericarditis After the Pfizer Messenger Ribonucleic Acid Coronavirus Disease Vaccine in Adolescents. Jenna Schauer, MD et al. Journal of Pediatrics. Published: July 02, 2021. 317-320.
[xxiv] https://childrenshealthdefense.org/defender/greyson-follmer-pfizer-vaccine-myocarditis
Exclusive: Athlete Who Recovered From COVID Facing ‘Very Different Future’ After Second Dose of Pfizer Vaccine Triggers Myocarditis. Megan Redshaw. The Defender Children’s Health Defense. June 21, 2021.
[xxv] https://expose-news.com/2022/06/04/athlete-deaths-18x-higher-than-expected
[xxvi] https://www.ahajournals.org/doi/abs/10.1161/circ.144.suppl_1.10712?s=09
Abstract 10712: Observational Findings of PULS Cardiac Test Findings for Inflammatory Markers in Patients Receiving mRNA Vaccines. Steven R Gundry. Circulation. Nov 8, 2021.
[xxvii] . https://openvaers.com/covid-data/myo-pericarditis.
VAERS COVID Vaccine Myo/Pericarditis Reports. (all vaccines) through July 22, 2022.
[xxviii] https://pubmed.ncbi.nlm.nih.gov/35148837
Immune imprinting, breadth of variant recognition, and germinal center response in human SARS-CoV-2 infection and vaccination. Katharina Röltgen and 42 co-authors. Cell. 2022 Mar 17;185(6):1025-1040.
[xxix] https://www.mdpi.com/1467-3045/44/3/73
Markus Aldén and 6 co-authors. Intracellular Reverse Transcription of Pfizer BioNTech COVID-19 mRNA Vaccine BNT162b2 In Vitro in Human Liver Cell Line. Curr. Issues Mol. Biol. 2022, 44(3), 1115-1126.
[xxx]https://onlinelibrary.wiley.com/doi/10.1111/andr.13209
Covid-19 vaccination BNT162b2 temporarily impairs semen concentration and total motile count among semen donors. Itai Gat, et al.. Andrology. 17 June 2022. 1-7.
[xxxi] https://www.theepochtimes.com/covid-jabs-impact-both-male-and-female-fertility_4619827.html?utm_source=ref_share&utm_campaign=web-cc-bright&utm_content=x&rs=SHRNQCKX&
COVID Jabs Impact Both Male and Female Fertility. Joseph Mercola. July 25, 2022.
Janci C. Lindsay Ph.D., Discusses Dangers of COVID JABS. Epoch Times.
[xxxii] https://www.commonsense.news/p/us-public-health-agencies-arent-following?s=r
U.S. Public Health Agencies Aren’t ‘Following the Science,’, Officials Say. Common Sense. Marty Makary, MD, MPH, and Tracy Beth Hoeg MD, Ph.D. July 14, 2022.
[xxxiii] Ibid.
[xxxiv] https://www.researchsquare.com/article/rs-1773983/v1
Association between School Mask Mandates and SARS-CoV-2 Student Infections: Evidence from a Natural Experiment of Neighboring K-12 Districts in North Dakota. Neeraj Sood, Shannon Heick, Josh Stevenson, Tracy Høeg.
[xxxv] https://www.law.cornell.edu/cfr/text/45/46.116
45 CFR 46.116 – General requirements for informed consent. Cornell Law School. Legal Informaton Institute.
[xxxvi] Neither Safe Nor Effective. The Evidence Against The CoVID Vaccines. © Dr. Colleen Huber. May, 2022. Chapter 14.
[xxxvii] https://globalcovidsummit.org/news/live-stream-event-physicians-alerting-parents
Global COVID Summit. Physicians and Medical Scientists. Full Text of Malone Statement.
Updated Jan 27, 2022. Original: Dec 11, 2021.
Bose Ravenel, MD, FAAP, Retired
Colfax, North Carolina
October 19, 2022

