Compiled by Bose Ravenel MD (pediatrician retired)
https://www.sciencedirect.com/science/article/pii/S221475002100161X
Volume 8, 2021, Pages 1665-1684
Why are we vaccinating children against COVID-19?
Ronald N.Kostoffa DanielaCalinab DarjaKanducc Michael B.Briggsd PanayiotisVlachoyiannopoulose Andrey A.Svistunovf AristidisTsatsakisg
Independent Consultant, Gainesville, VA, 20155, USA
Department of Clinical Pharmacy, University of Medicine and Pharmacy of Craiova, 200349, Craiova, Romania
Department of Biosciences, Biotechnologies and Biopharmaceutics, University of Bari, Italy
Independent Consultant, Roscommon, MI, 48653, USA
Department of Pathophysiology, Medical School, National and Kapodistrian University of Athens, Athens, Greece
Department of Pharmacology, I.M.Sechenov First Moscow State Medical University (Sechenov University), 119146, Moscow, Russia
Department of Forensic Sciences and Toxicology, Faculty of Medicine, University of Crete, 71003, Heraklion, Greece
Received 16 July 2021, Revised 11 August 2021, Accepted 29 August 2021, Available online 14 September 2021.
Highlights
- Bulk of COVID-19 per capita deaths occur in elderly with high comorbidities.
- Per capita COVID-19 deaths are negligible in children.
- Clinical trials for these inoculations were very short-term.
- Clinical trials did not address long-term effects most relevant to children.
- High post-inoculation deaths reported in VAERS (very short-term).
Note:
The following section is comprised of sections from the report italicized
Medical treatment, not a vaccine
A vaccine is legally defined as any substance designed to be administered to a human being for the prevention of one or more diseases [5 ].. . In the remainder of this article, we use the term ‘inoculated’ rather than vaccinated, because the injected material in the present COVID-19 inoculations prevents neither viral infection nor transmission. Since its main function in practice appears to be symptom suppression, it is operationally a “treatment”.
CoVID-19 Death numbers artificially inflated
By the end of May 2021, the official CDC death count attributed to COVID-19 was approaching 600,000, as stated previously. This number has been disputed for many reasons. First, before COVID-19 testing began, or in the absence of testing, after it was available, the diagnosis of COVID-19 (in the USA) could be made by the presumption of the healthcare practitioner that COVID-19 existed [4,18]. Second, after testing began, the main diagnostic used was the RT-PCR test. This test was done at very high amplification cycles, ranging up to 45 [[19], [20], [21]]. In this range, very high numbers of false positives are possible [22].
Third, most deaths attributed to COVID-19 were elderly with high comorbidities [1,22]. As we showed in a previous study [22], attribution of death to one of many possible comorbidities or especially toxic exposures in combinations [23] is highly arbitrary and can be viewed as a political decision more than a medical decision. For over 5 % of these deaths, COVID-19 was the only cause mentioned on the death certificate. For deaths with conditions or causes in addition to COVID-19, on average, there were 4.0 additional conditions or causes per death [24]. These deaths with comorbidities could equally have been ascribed to any of the comorbidities [22]. Thus, the actual number of COVID-19-based deaths in the USA may have been on the order of 35,000 or less, characteristic of a mild flu season.
Even the 35,000 deaths may be an overestimate. Comorbidities were based on the clinical definition of specific diseases, using threshold biomarker levels and relevant symptoms for the disease(s) of interest [25,26]. But many people have what are known as pre-clinical conditions. The biomarkers have not reached the threshold level for official disease diagnosis, but their abnormality reflects some degree of underlying dysfunction. The immune system response (including pre-clinical conditions) to the COVID-19 viral trigger should not be expected to be the same as the response of a healthy immune system [27]. If pre-clinical conditions had been taken into account and coupled with the false positives as well, the CDC estimate of 94 % misdiagnosis would be substantially higher.
CoVID deaths per capita in US for children vanishingly low
Fig. 1 uses the official large CDC numbers (coupled with USA census data estimates from CDC Wonder) to show the COVID-19 deaths per capita as a function of age, circa early June 2021. Unfortunately, the most critical range, 85+, has the least resolution. It is obvious that most of the deaths occurred in the 55 to 100+ range, and the remaining individuals in the other ranges (especially under 35) have negligible risk of dying from the disease.
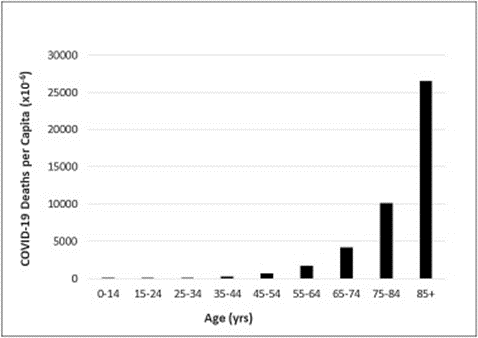
Fig. 1. COVID-19 Deaths per capita by age in the United States (as of Jun 5, 2021). Population-based on U.S. CDC WONDER Bridge-Race Population Estimate 2019. Data obtained from https://wonder.cdc.gov/bridged-race-v2019.html on 6/15/2021. Provisional COVID-19 deaths based on CDC data provided by the National Center for Health Statistics for the period 1/1/2020 – 6/5/2021. Data obtained from https://data.cdc.gov/NCHS/Provisional-COVID-19-Deaths-by-Sex-and-Age/9bhg-hcku on 6/10/2021.
FDA EUA authorization based upon short-term, no long-term data
However, symptoms/diseases are typically end points of processes that can take months, years, or decades to surface. . . .
Instead, in the absence of high-quality safety science reflected in these experiments, all that could be determined were short-term adverse effects and deaths.
3.1.3.1. Intrinsic inoculant toxicity
Children are unique relative to COVID-19. They have negligible risks of serious effects from the disease, as shown in Fig. 1. Given that the COVID-19 inoculants were only tested for a few months, and mid-or long-term adverse effects are unknown, any mid- or long-term adverse events that emerge could impact children adversely for decades.
Deaths following inoculation cluster heavily supporting causal relationship
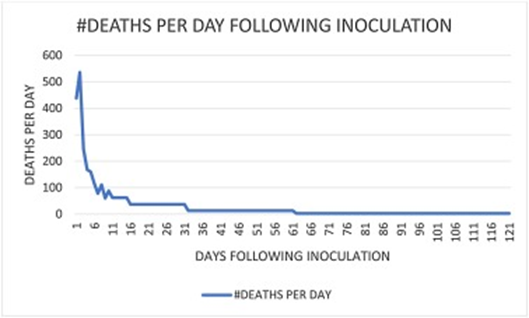
Fig. A1. Figure A1-1 is a plot of number of deaths from COVID-19 inoculation (reported to VAERS and obtained from the CDC search engine CDC Wonder) as a function of days from inoculation (zero reflects day of inoculation). If there were no effect from the inoculation, as claimed by the CDC and other official government agencies, the curve would be essentially a straight horizontal line, reflecting normal expected deaths in a non-COVID-19 year.
Adverse CoVID vaccine effects on children
3.1.3.2. Adverse inoculant effects on children
What are the potential mid- and long-term adverse health effects from the COVID-19 inoculation on children specifically, taking into account that they will be exposed not only to the spike protein component of the SARS-CoV-2 virus but also to the toxic LNP encapsulating-shell? This toxic combination will have bypassed many defensive safeguards (typically provided by the innate immune system) through direct injection [62]. As we have shown, the main reasons why we believe the spike protein could be harmful to children even though they don’t seem to get sick from exposure to SARS-CoV-2 are 1) the bypassing of the innate immune system by inoculation, 2) the larger volume of spike protein that enters the bloodstream, and 3) the additional toxic effects of the encapsulating LNP layer.
. . . .
What is the rush for a group at essentially zero risks? Given that the inoculations were tested only for a few months, only very short-term adverse effects could be obtained. It is questionable how well even these short-term effects obtained from the clinical trials reflect the short-term effects from the initial mass inoculation results reported in VAERS.
Fig. 1, Fig. 2 reflect only these very short-term results. A number of researchers have suggested the possibility of severe longer-term autoimmune, Antibody-Dependent Enhancement, neurological, and other potentially serious effects, with lag periods ranging from months to years. If such effects do turn out to be real, the children are the ones who will have to bear the brunt of the suffering. There appear to be no benefits for the children and young adults from the inoculations and only Costs!
In the Conclusions section, the authors had this to say:
As stated before, CDC showed that 94 % of the reported deaths had multiple comorbidities, thereby reducing the CDC’s numbers attributed strictly to COVID-19 to about 35,000 for all age groups. Given the number of high false positives from the high amplification cycle PCR tests, and the willingness of healthcare professionals to attribute death to COVID-19 in the absence of tests or sometimes even with negative PCR tests, this 35,000 number is probably highly inflated as well.
On the latter issue, both Virginia Stoner [85] and Jessica Rose [86] have shown independently that the deaths following inoculation are not coincidental and are strongly related to inoculation through strong clustering around the time of injection. Our independent analyses of the VAERS database reported in Appendix 1 confirmed these clustering findings.
Additionally, VAERS historically has under-reported adverse events by about two orders-of-magnitude, so COVID-19 inoculation deaths in the short-term could be in the hundreds of thousands for the USA for the period mid-December 2020 to the end of May 2021, potentially swamping the real COVID-19 deaths. Finally, the VAERS deaths reported so far are for the very short term. We have no idea what the death numbers will be in the intermediate and long-term; the clinical trials did not test for those.